What is Coarctation of the Aorta?
Coarctation of the aorta is a congenital heart defect, or a birth defect of the heart. It involves a narrowing of the aorta, the main blood vessel carrying oxygen-rich blood from the left ventricle of the heart to all of the organs of the body. Coarctation occurs most commonly in a short segment of the aorta adjacent to the ductus arteriosus. The ductus arteriosus is a blood vessel normally present in all fetuses that forms a connection between the pulmonary artery and the aorta. The ductus arteriosus has special oxygen-sensing tissue in its wall that causes it to close in the first hours or days of life. It is thought that coarctation may be caused by the presence of extra ductal tissue extending into the adjacent aorta which results in aortic narrowing as the ductal tissue contracts.
Incidence
Congenital heart defects occur in 1 out of every 150 pregnancies, and coarctation of the aorta represents up to 5% of these defects. The overall incidence is about 5 in 10,000 births. Coarctation may occur in isolation or in association with other heart defects involving the left side of the heart, such as a bicuspid aortic valve, aortic valve stenosis, or ventricular septal defect. Coarctation may also be seen as a part of more complex defects, such as hypoplastic left heart syndrome. Coarctation of the aorta is common in patients with some chromosomal abnormalities, such as Turner's syndrome.
Cause
The cause of coarctation of the aorta is unknown. Genetic factors may play a role. Some experts believe that elastic tissue from the ductus arteriosus may encircle the aorta and cause a "lasso effect" on it as the ductus closes, resulting in a coarctation of the aorta .
Signs and Symptoms
The symptoms of coarctation of the aorta depend on the severity of the narrowing. In approximately 50 percent of cases of isolated coarctation, the narrowing is severe enough to cause symptoms in the first few days of life when the ductus arteriosus closes. When the ductus arteriosus closes, the left ventricle must suddenly pump against much higher resistance which can lead to symptoms of heart failure or shock, such as rapid breathing, sweating, or lethargy. Because these newborns are well up until the ductus arteriosus closes, symptoms appear rapidly and are often severe.
In mild cases of coarctation, symptoms may be subtle and the diagnosis may not be made for several years. After infancy, the most frequent findings leading to the detection of coarctation are a heart murmur, diminished lower extremity pulses, or high blood pressure in the arms. Symptoms such as chest pain, palpitations, or syncope are unusual in the setting of coarctation of the aorta.
Diagnosis
Occasionally a coarctation of the aorta may be suspected before birth through the use of a fetal echocardiogram. After birth, the diagnosis of coarctation is usually made with an echocardiogram, which can define the anatomy of the aorta and evaluate for other cardiac anomalies. Occasionally in older children the region of coarctation is difficult to image well by echocardiography. In such cases, MRI or CT scan may be used. Cardiac catheterization is occasionally necessary for diagnosis.
Treatment
In a critically ill newborn, a continuous intravenous medication, prostaglandin (PGE-1), is used to open the ductus arteriosus allowing blood to flow to areas beyond the coarctation. Once the patient is stabilized, usually coarctation surgery is performed. The severity and length of the coarctation segment will dictate the most appropriate technique.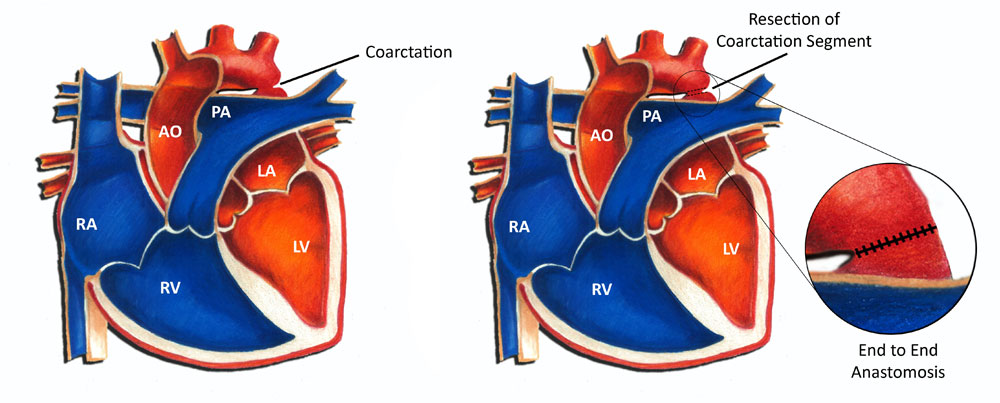
Occasionally in older children catheter-based therapy may be a possible alternative to surgery. In selected cases, the area of narrowing may be dilated and stented with a balloon. The characteristics of the narrowing and the age of the child are considered in deciding if stent placement is an option for treatment.
Prognosis
Long-term prognosis following coarctation repair is excellent, although recurrence of coarctation at the area of the repair is possible, even years following treatment. The rate of restenosis is highest among newborns, and decreases in older children. While surgery may be necessary for some patients for recurrence, the majority of cases and be managed with cardiac catheterization and balloon dilation as the initial approach. Another concern after coarctation repair is high blood pressure. The chances of having chronic high blood pressure requiring treatment are greater the older a child is at the time of repair. Long-term follow-up with a cardiologist is important for children after coarctation repair to diagnose late problems of restenosis or hypertension. Another reason continued follow-up is important is because approximately 30 percent of patients with coarctation also have a bicuspid aortic valve. Such a valve abnormality may lead to problems later in life.
In summary, coarctation of the aorta, although a potentially serious heart problem, is very treatable with excellent outcomes in this day and age.